Sidebar






")

Research News
Decolonizing Global Health : Know Your Organizational Weaknesses
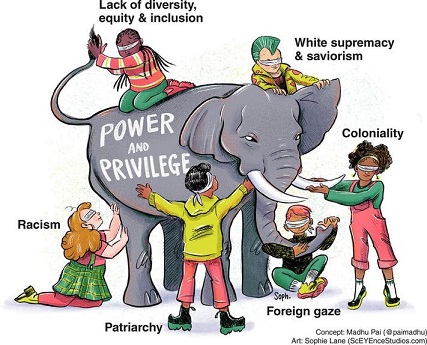 In an interesting interview for Global Health Now (GHN), Carel IJsselmuiden and James Lavery share their view on "how the RFI speaks to the need for organizations to reflect and take stock of any shortcomings". The RFI isn’t a report card that brands institutions as good or bad. It’s intended, instead, to provide a pathway to self-improvement—which is the essence of decolonization.
In an interesting interview for Global Health Now (GHN), Carel IJsselmuiden and James Lavery share their view on "how the RFI speaks to the need for organizations to reflect and take stock of any shortcomings". The RFI isn’t a report card that brands institutions as good or bad. It’s intended, instead, to provide a pathway to self-improvement—which is the essence of decolonization.
(Ref: Joanne Silberner for Global Health NOW)
Find out if you're a Colonizer or Decolonizer
[Announcement:]: Free Mini Certificate in Health Research Ethics for Students

Free ethics training for students in health research ethics!
The 12-hour virtual training is very interactive and features more than 20 experts in bioethics from the APRU network. This year it will take place on April 14/15, April 28/29, and May 13/14.
Space is limited and the deadline to register is April 10, 2022.
‘Working relationships’ across difference - a realist review of community engagement with malaria research
Abstract
Background: Community engagement (CE) is increasingly accepted as a critical aspect of health research, because of its potential to make research more ethical, relevant and well implemented. While CE activities linked to health research have proliferated in Low and Middle Income Countries (LMICs), and are increasingly described in published literature, there is a lack of conceptual clarity around how engagement is understood to ‘work’, and the aims and purposes of engagement are varied and often not made explicit. Ultimately, the evidence base for engagement remains underdeveloped.
Methods: To develop explanations for how and why CE with health research contributes to the pattern of outcomes observed in published literature, we conducted a realist review of CE with malaria research – a theory driven approach to evidence synthesis.
Results: We found that community engagement relies on the development of provisional ‘working relationships’ across differences, primarily of wealth, power and culture. These relationships are rooted in interactions that are experienced as relatively responsive and respectful, and that bring tangible research related benefits. Contextual factors affecting development of working relationships include the facilitating influence of research organisation commitment to and resources for engagement, and constraining factors linked to the prevailing ‘dominant health research paradigm context’, such as: differences of wealth and power between research centres and local populations and health systems; histories of colonialism and vertical health interventions; and external funding and control of health research.
R&D : More Than Sharing Vaccines
"This pandemic is not over until it is over everywhere."
A commentary by COHRED's Executive Director, Board members, associates and partners published in Think Global Health highlights a complete change is needed in the approach to and funding of global preparedness.
Regardless of an increasing provision of vaccines, there are many of the poorest countries, health and research and development (R&D) systems are absolutely lacking to serve the needs of their populations. Although some are privileged to live in countries with effective health research and development systems that can ramp up their responses to such emergencies, many are not. This R&D inequity lies at the core of current and future lost lives.
The COVID-19 pandemic underlines the vaccine inequity is ethically wrong. Its continuation for more than two years into the pandemic shows the limits of global solidarity as an effective global public health strategy. For several decades, most LMICs have invested low in their own R&D ecosystems and remain depended on the scientific, and financing efforts of high-income countries to address their R&D requirements which does not solve the long-term problem of inequitable participation in effective R&D and resulting interventions.
The two biggest current threats to global health security—pandemics and climate change—require equitable access to R&D and implementation.
"Vaccine inequity" should not become "vaccination inequity."
R&D equity should become an explicit objective in national and international development and collaboration policy, especially between high- and low- and middle-income countries.
Mental health and well-being of children in the Philippine setting during the COVID-19 pandemic
Abstract
The coronavirus disease 2019 (COVID-19) pandemic has subjected the mental health and well-being of Filipino children under drastic conditions. While children are more vulnerable to these detriments, there remains the absence of unified and comprehensive strategies in mitigating the deterioration of the mental health of Filipino children. Existing interventions focus on more general solutions that fail to acknowledge the circumstances that a Filipino child is subjected under. Moreover, these strategies also fail to address the multilayered issues faced by a lower-middle-income country, such as the Philippines. As the mental well-being of Filipino children continues to be neglected, a subsequent and enduring mental health epidemic can only be expected for years to come.
Keywords: Mental Health, Philippines, COVID-19, Psychology, Child, Child care, Health services, Social problems
More Articles ...
Research News
- Call for Research Abstracts: Healthy Aging Summit 25
- Second Call for Applications: 2025 DOST-PCHRD Undergraduate Thesis Grant in Natural Products
- FREE WEBINAR: "EVIDENCE AT THE CORE: BUILDING RESILIENT POLICIES FOR HEALTH AND EDUCATION"
- Invitation for Free Training on Digital Toolkit and Integrating OMICS Technology
- CALL FOR ENTRIES: 2025 ClusteRICE
- DOST-PCHRD 2025 CFA: PhD in Molecular Biomedicine (Trieste, Italy)
- Call for Participants: Good Clinical Practice (GCP) Training
- 5th DOST-PCHRD Webinar and Workshop for Early Career Researchers
- VISUAL ABSTRACT CONTEST
- DOST-PCHRD 2024 Call for Applications: MSc/PhD in Tropical Medicine (Mahidol University, Thailand)
- NPGP Bulletin No. 2024-01: Dissemination of 2023 National Practice Guidelines
- FIGO statement: Fertility preservation
- Geneva Sustainability Centre launches Sustainability Accelerator Tool for hospitals
- Filipino researchers develop newborn screening device for early detection of hearing impairment
- [DOST-PCHRD] Call for Proposals: IPROTECH, TEKI in Health, & Start Up Research Grant Program
- IHF Awards: Deadline for entries is extended to 30 June
- IHF Awards 2023 | Call for entries now open!
- Call for abstracts now open! | 46th World Hospital Congress
- Chronic pain: Non-opioid drug candidates could offer relief without addiction
- 8th BSP Convention 2022
- Serpentina Capsule with antioxidant/anti-inflammatory health benefits
- DLSU-IBEHT’s Agapay Project secures its first patent certificate
- Food allergy is associated with lower risk of SARS-CoV-2 infection
- Children from historically marginalized groups or poor backgrounds less likely to survive neuroblastoma
- Decolonizing Global Health : Know Your Organizational Weaknesses
- [Announcement:]: Free Mini Certificate in Health Research Ethics for Students
- ‘Working relationships’ across difference - a realist review of community engagement with malaria research
- R&D : More Than Sharing Vaccines
- Mental health and well-being of children in the Philippine setting during the COVID-19 pandemic
- Disconnected perspectives: Patient and care provider's experiences of substance use in pregnancy
- Invitation to the 7th World Conference on Research Integrity
- EVALUATING DIGITAL AND TECHNOLOGY-DRIVEN TRANSFORMATIONS IN HEALTHCARE: TAKING THE SOFT APPROACH
- Free Mini Certificate in Health Research Ethics for APRU Students
- Call for Proposals: 2022 AHEAD - HPSR
- International Atomic Energy Agency (IAEA) Marie Sklodowska-Curie Fellowship Program
- In-Dept Assessment of the Causes and Effects of Adolescent Pregnancy in Regions I, VII, and XI in the Philippines (2021)
- Neuroscience reveals how a year of social distancing broke our brains
- Equity in Science Funding
- Call for Workshop Applicants-Using Mathematical Modeling to Aid Governance in Universal Health Care in the Philippines
- [Invitation] Research Fairness Webinar: Equitable Partnerships in Science, Technology, and Innovation
- IHF World Hospital Congress Call for Abstracts re-opens in March
- IHF YOUNG EXECUTIVE LEADERS
- Building the New Normal: Harnessing Transformative Practices from the COVID-19 Pandemic
- TOWARDS POST-COVID-19: SUCCESS STORIES AND LESSONS LEARNED FOR THE FUTURE
- Call for applicants for 1st WHO training in infodemic management
- Framework for Reopening Schools
- New COVID-19 Law Lab to provide vital legal information and support for the global COVID-19 response
- Ethical Considerations for Resuming In-Person Interactions with Healthcare Professionals Post COVID-19: A Guidance Document
- Filling the Gaps: Learning From Each Other During the COVID-19 Pandemic
- Virtual health care in the era of COVID-19
- Hospital beds and coronavirus test centres are needed fast. Here’s an Australian-designed solution
- Global coalition to accelerate COVID-19 clinical research in resource-limited settings
- (Policy Brief) Potential Economic Effects of Lockdown in the Philippines due to COVID-19: Lessening the Impact on Poor Households
- Research Priority to Fight COVID-19 | COHRED Executive Director's Message
- Health Research Capacities in Palestine: High-quality and Proper Knowledge Transfer and Translation for Sound Decision-making
- UP-NIH 22nd Anniversary: HEALTH AMIDST CLIMATE CHANGE, DISASTERS AND OUTBREAKS
- WHO Guideline: Recommendations on Digital Interventions for Health System Strengthening
- Report on the WHO WESTPAC Regional Conference
- IHF Journal Volume 55 Number 3
- Philippines to spend $17b on health
- R1HRDC Funded Research Now Available on Amazon
- WHO Celebrates World Humanitarian Day
- Measure what matters most in healthcare—value, affordability and outcomes
- Price setting and price regulation in health care (Lessons for advancing universal health coverage)
- ANTI MICROBIAL RESISTANCE - Turning plans into action working paper
- Release of the IHF Journal Volume 55 No. 2
- Accreditation and culture usually go hand-in-hand in health organisations
- One in four health care facilities lacks basic water services, say WHO and UNICEF
- ASEAN-India Research Training Fellowship (AIRTF) for 2019
- Implementation fidelity of a strategy to integrate service delivery: learnings from a transitional care program for individuals with complex needs in Singapore
- Social innovation in health: leaving no one behind
- Public Spending on Health: A Closer Look at Global Trends
- IHF World Hospital Congress CALL FOR ABSTRACTS
- International Hospital Federation Official Journal 2018 Volume 54 Number 4
- International Hospital Federation Official Journal 2018 Volume 54 Number 3
- A systematic approach to develop a core set of parameters for boards of directors to govern quality of care in the ICU
- CARE NEEDED: Improving the Lives of People with Dementia
- Measuring Health and Economic well being in the Sustainable Development Goals Era
- What is the experience of decentralized hospital governance in Europe?
- TRANSFORMING HEALTH CARE DELIVERY Achieving Better Outcomes and Affordability
- How responsive is the Philippine Health Care System? (©DOH 2018 AHEAD-HPSR)
- How can we get quality evidence in the hands of decision makers in a timely manner? (©DOH 2018 AHEAD-HPSR)
- Hot Topic: Urgency of Another Sin Tax Reform (©DOH 2018 AHEAD-HPSR)
- What Factors Influence Drug Pricing in Public Hospitals? (©DOH 2018 AHEAD-HPSR)
- Updates on the Universal Health Care Act (©DOH 2018 AHEAD-HPSR)
- Are Health Services Reaching Filipinos Living in Slums?(©DOH 2018 AHEAD-HPSR)
- How can the Health Sector consistently produce high quality Clinical Practice Guidelines (CPGs)? (©DOH 2018 AHEAD-HPSR)
- How Should PhilHealth Set the Case Rates? Lessons from A Costing Study (©DOH 2018 AHEAD-HPSR)
- Online Grant Writing Workshop for Early and Mid-Career Researchers
Featured Links
PNHRS

PCHRD

eHealth

Ethics

ASEAN-NDI
